Retinopathy of Prematurity Detection and Treatment

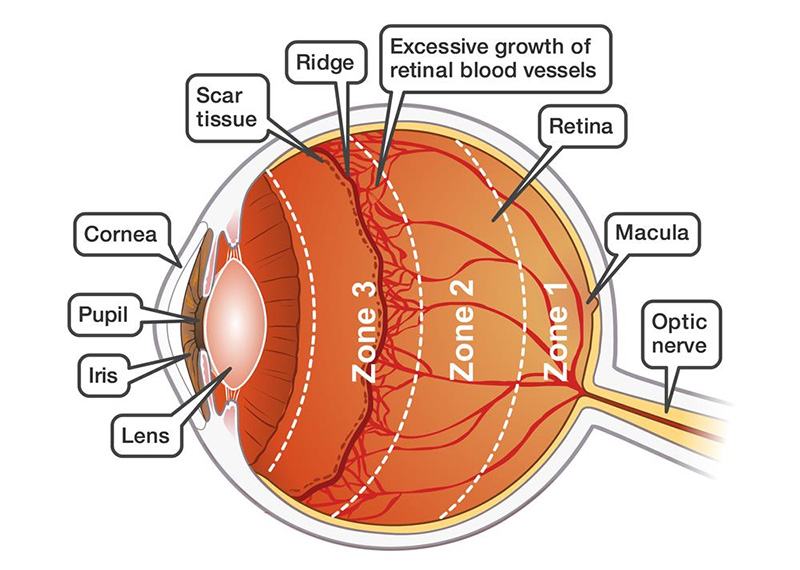
Retinopathy of prematurity (ROP) is a condition associated with abnormal retinal vascular development in babies born at or before 30 weeks of gestation.
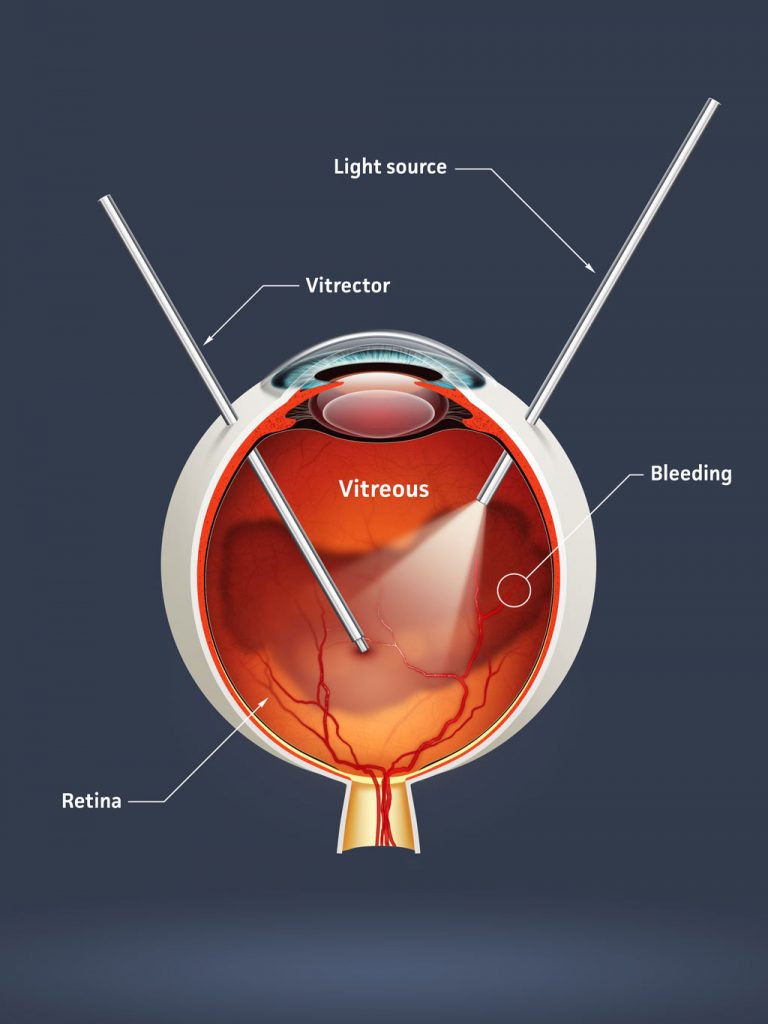
Advanced stages of ROP may require treatment, although this is not always the case. Milder stages are very common, and most affected newborns will recover completely. However, if advanced cases remain untreated, it can lead to blindness.
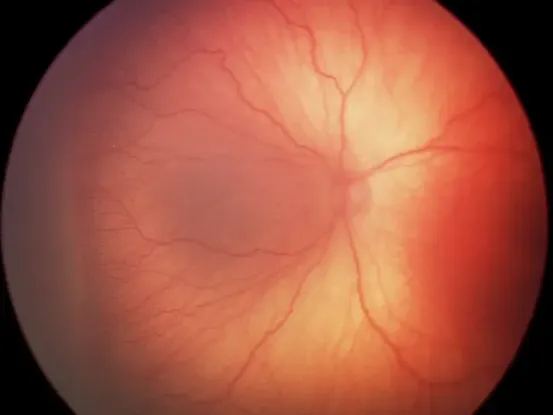
The most effective method of detecting ROP in premature infants is through regular screening, and this should continue until the retina has fully vascularised.
Babies who are born prematurely or those who develop any stage of ROP can develop other eye conditions like strabismus, amblyopia or refractive errors later in life. Therefore, they should be assessed regularly by a paediatric ophthalmologist to monitor the potential development of these conditions after they turn one.